

In November last year, an influential coalition of housing and charity groups, including RIBA and Age UK, said that “the next Government should make all new homes accessible and adaptable”. The open letter went on to say: “Without action, we face an ever-mounting bill, with councils spending greater sums on trying to adapt homes retrospectively and the costs to our health and social care systems spiralling”.
Smartlouvre





Air conditioning is a relatively new invention that is becoming required more and more to manage the temperature in buildings. We all know that we’re spending increasing amounts of time indoors, avoiding the elements, and whilst we do, the fact is, we are damaging those elements.
One question that I’ve asked myself and my peers many a time is why are we not building better, to accommodate the effects of the elements? The answer is always a wide range of justifications to the fact that we are. My argument in response is that in a lot of cases, we’re avoiding the obvious. To build with the effect of the elements in mind, we’re utilising technology in cooling that does quite the opposite.
Hospitals and hospices are the biggest contradiction. In a healthcare environment, the occupants need daylight more than ever. I don’t need to harp on about the benefits. A connection to the outdoors and having access to natural light helps patients heal faster, making for a shorter hospital stay, and in general, the therapeutic environment that is strived for.
So, whilst one would assume methodology for optimising daylight was applied in the initial phases of the building design, what were the architect’s/client’s overriding decision factors for the final design? Because there’s always a compromise.
Was it high levels of daylight alone? Energy efficiency? Or a combination of both?
But what about managing the heat that the daylight also provides? Mitigating glare? Always a secondary factor in my experience. All too often disregarded, or at least deprioritised and found to be a problem after the building is occupied – by those who most need visual and thermal comfort, and those who are trying to care for them, in uncomfortable temperatures. And so, the facilities manager takes on the burden.
Back in 2018, a UK heatwave saw NHS trusts bulk-buying mobile air-conditioning units, fans and bottled water to help beat the negative effect of temperatures, which climbed to up to 40C inside wards. It’s a widespread problem, only expected to get worse. 2020 is predicted to be the warmest year in UK history when we are also dealing with a global coronavirus pandemic.
The pandemic brings this building cooling issue to the forefront. Cibse guidance is clear; we should wherever possible, enable the natural ventilation of buildings
by opening windows and not use methods of cooling air by recirculation.
Hospitals are complex builds to deliver; no-one would deny that. So, is that why solar shading isn’t prioritised? Or is it the cost of cooling? Or the effect on the environment that overrides? After all, installation of air conditioning uses large amounts of energy and contributes to climate change. Ventilation is needed, especially whilst dealing with the pandemic, but so is heat and light control.
Worse still, healthcare trusts which don’t have imminent budgets for new buildings are seeing their running costs rise, year after year, in order to manage temperatures in buildings built when these levels of temperatures weren’t even a consideration.
The Committee on Climate Change (the Government’s official climate change advisors) stated in a recent report that the types of hospital ward that are vulnerable to overheating currently make up 90% of the total stock (by floorspace). A recent Cambridge University report found that some £17.5bn of upgrades could be needed to make UK hospitals resilient to the heat through new shading measures and improved ventilation. Overheating in hospitals is a serious issue.
The general design guidance for healthcare premises as defined by the Department of Health isn’t prescriptive when it comes to solar gain and glare. It simply states that it should be controlled and suggests examples of providing control being through louvres and blinds. Internal or external, it doesn’t say. Furthermore, it suggests that thermal comfort conditions are ‘issues to consider’. Where are the standards? The minimum heat gain and glare, the temperatures acceptable at any given point in the day? Recuperating patients require a lot of sleep, which is interrupted at just 26C, and that’s just the start.
And so, the management of heat and glare is left to shading solutions that at best, remove only some of the problems, or at worst, also remove the benefits of the glazing and/or the daylight.
Internal blind systems remove visibility and a connection with the outside world and only protect the room from a minimal amount of heat gain. External shading systems do work but are expensive to install and maintain as well as reducing the quality of daylight. Even the most recent advances in glazing technology reduce the view out.
So, what is the answer? How do you get optimum daylight distribution, visibility to the outside world, protection from glare and the opportunity for ventilation?
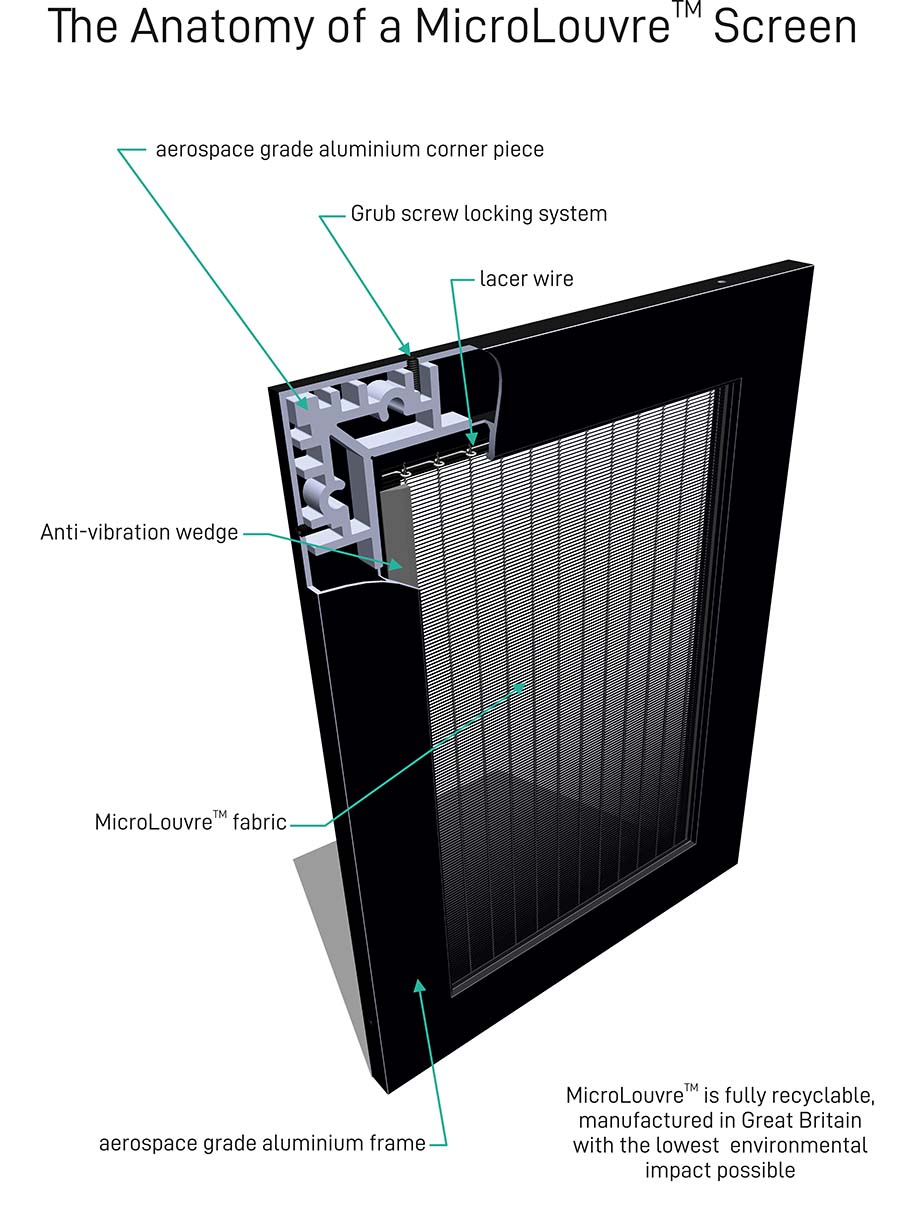
You stop the heat and light before it hits the glass, with a metal fabric, with micro-fine louvres woven in to dissipate the sun’s heat and energy but not block natural daylight, natural ventilation or vision out.
This solution works totally differently from traditional external and internal blinds, which reflect, distort and restrict vision and light, MicroLouvre fabric simply and invisibly neutralises solar heat gain and glare before they even reach the window, working non-stop like a heat exchanger dissipating the sun’s heat and energy into the atmosphere.
It doesn’t diffuse daylight; it provides all the benefits but not the negative impact of excessive heat gain and glare. The louvres are micro-fine, and angled at a level to ensure optimum light in, and visibility out, whilst protecting the building occupants from the heat, glare and even external viewing in. It’s known as angular selective technology.
The performance of this fabric has been tested, time and time again by standards agencies, scientists and researchers, including the BRE. It’s not a fly-by-night product either. It’s been around since the 1940s, but in recent years, it’s been honed, and the production process improved so that it remains the best solution for solar shading I’ve seen in my 45(ish) years in the business.


